Fishman commentary: Treatment pearls for dupilumab associated ocular surface disease.
Authors: JodieRaffiabRaaginiSureshaTimothyBergeraHarveyFishmancJenny E.Murasead
https://doi.org/10.1016/j.ijwd.2019.08.007 International Journal of Women’s Dermatology . Available online 24 August 2019.
Atopic dermatitis is associated with a range of ocular complications. Additionally, an increase in dupilumab-associated conjunctivitis, dry eye, and recently characterized residual ocular surface disease has been demonstrated in multiple studies. Given recent evidence that interleukin-4 and -13 may play a role in goblet cell proliferation and mucous secretion (Garcia-Posadas et al., 2018), blockage of these particular immune pathways by dupilumab may ultimately lead to tear film instability and dry eye.
Individuals who use chronic steroid eyedrops are at risk for the development of adverse effects, including glaucoma, cataracts, decreased wound healing, and orbital fat atrophy, and need to be followed by an ophthalmologist. Significant relief can be achieved with a nonsteroid ophthalmologic regimen after an initial pulse treatment of topical steroids initiated by an ophthalmologist.
Therapeutic pearl
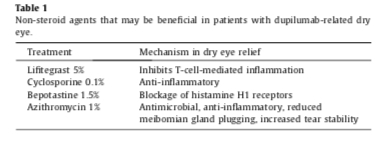
The primary initial goal of treatment is to improve meibomian gland function with eyelid hygiene, warm compresses, oral omega-3 fatty acid supplementation, and azithromycin ophthalmic solution 1% (Azasite), an antibiotic that exhibits anti-inflammatory effects, enhances meibum production, and improves tear stability. After eyelid inflammation is controlled, additional topical ophthalmological treatments to reduce inflammation and enhance the tear film can be introduced. Lifitegrast 5% ophthalmic solution inhibits T-cell-mediated inflammation by blocking the interaction between the ligand intercellular adhesion molecule-1 and lymphocyte function–associated antigen-1.
Cyclosporine 0.1% ophthalmic emulsion is another anti-inflammatory agent that can be used safely in conjunction with lifitegrast for treatment of chronic dry eye (Zirwas et al., 2018). Bepotastine 1.5% solution is an antihistamine that relieves the pruritus and redness associated with dry eye by blocking histamine H1 receptors, stabilizing mast cells, and preventing degranulation. Other antihistamines that may be used are azelastine 0.05% solution, epinastine 0.05% solution, alcaftadine 0.25% solution, and olopatadine. 0.1% solution (taking into consideration that antihistamine drops may exacerbate dry eye while alleviating ocular pruritus).
We have used a combination of these four agents at twice daily dosing with significant relief in patients with dupilumab-associated dry eye (Table 1).
References
- Garcia-Posadas et al., 2018
-
L. Garcia-Posadas, R.R. Hodges, Y. Diebold, D. DarttContext-dependent regulation of conjunctival goblet cell function by allergic mediatorsSci Rep, 8 (2018), p. 12162
- Zirwas et al., 2018
-
M.J. Zirwas, K. Wulff, K. BeckmanLifitegrast add-on treatment for dupilumab-induced ocular surface disease (DIOSD): a novel case reportJAAD Case Rep, 5 (1) (2018), pp. 34-36


